Do We Really Need Pills Morning, Noon and Night?
What if one injection or a tiny patch on the skin could replace the daily routine of swallowing pills? Researchers are racing to develop long acting medicines for people with chronic disease. The promise is clear. The challenges are not.
Before meals. After meals. At night. For seven days. On an empty stomach.
Anyone who has ever picked up a prescription knows the drill: detailed instructions, carefully explained. And just as familiar is the reality that follows. Over time, many of us drift away from the plan. In fact, up to 80 per cent of Danes do not follow long‑term treatment regimens exactly as prescribed.
The result is often too little medicine or too much. Treatments become less effective, while patients and public healthcare systems alike pay the price. But what if future medicines didn’t depend on memory at all? What if a single injection could last months – or even years? For some, that idea feels unsettling. For others, it sounds like freedom.
Long‑acting “depot” medicines already exist for certain conditions, including schizophrenia, HIV, prostate cancer, opioid dependence and hormone‑sensitive diseases. But researchers hope that similar approaches could one day be used to treat conditions such as dementia, malaria, tuberculosis and depression – or to provide long‑term contraception.

The Hidden Waste in a Pill
Even when we take pills exactly as instructed, the process itself is surprisingly crude. Swallow a tablet, and the concentration of the active substance in the body spikes – then steadily drops until the next dose. To ensure adequate coverage throughout the day, pills are formulated with much more medicine than the body actually needs.
“When medicine is taken orally, the concentration of the active compound can be twice what’s required,” explains René Holm. “The surplus isn’t used – it’s excreted, mainly through faeces – and it can end up in the environment. We manufacture more, and discard more, than is necessary.”
This, he says, is the sustainability problem. Overproduction is costly not only for healthcare budgets, but also for nature. Studies have shown worrying levels of pharmaceutical residues – particularly antibiotics, antidepressants and painkillers – in Danish rivers, lakes and coastal waters.
From ‘Problem Patients’ to Preferred Treatment
Depot medicines are not a recent invention. The first entered the market in 1966, when the antipsychotic fluphenazine enanthate was introduced as an injection given every one to three weeks. Two years later, fluphenazine decanoate extended that interval to up to four weeks. Today, some people with schizophrenia require just one injection every six months.
Since then, pharmaceutical science has advanced dramatically. Active compounds can now be encapsulated in biodegradable polymers, allowing researchers to control precisely how much medicine is released and when. What was once seen as a last resort for “difficult” patients has become a genuine alternative to daily tablets.
Still, Holm stresses, depot medicines are not suitable for everything.
“They make particular sense for chronic and often stigmatizing diseases,” he says. “Conditions you don’t necessarily want to be reminded of twice a day. HIV is a good example: it can now be treated with injections given only twice a year.”
Why Pills Are Still with Us
If scientists have become so good at designing long‑acting medicines, why are we still taking pills three times a day?
The answer is partly mundane. Some active substances are simply too bulky. Others are unstable. And some stubbornly resist all attempts at pharmaceutical fine‑tuning. Nature, it turns out, sets hard limits.
“Sometimes we have to accept defeat because the technical hurdles are just too high,” Holm says. “Right now, we’re working with pretomanid, a crystalline compound used to treat tuberculosis. And it really is a tough case.”
When Nature Refuses to Cooperate
Pretomanid is a source of both frustration and fascination. It refuses to behave – and yet, in doing so, it showcases nature’s engineering at its finest.
“It’s a crystal that is extremely comfortable with itself,” Holm says, “It’s incredibly hard and has absolutely no interest in being broken down into the smaller particles we need. It’s simply too stable.”
For pretomanid to work as a depot medicine, it must be reduced to much smaller particles; otherwise, each dose becomes too large. But the bonds holding the crystal together are so strong that approved pharmaceutical methods can’t break it down far enough. The material simply isn’t brittle enough. Milling it is like trying to grind granite into flour.
“We can’t get the particles below five micrometres, and that’s not small enough. So we have to explore entirely different formulation strategies.”
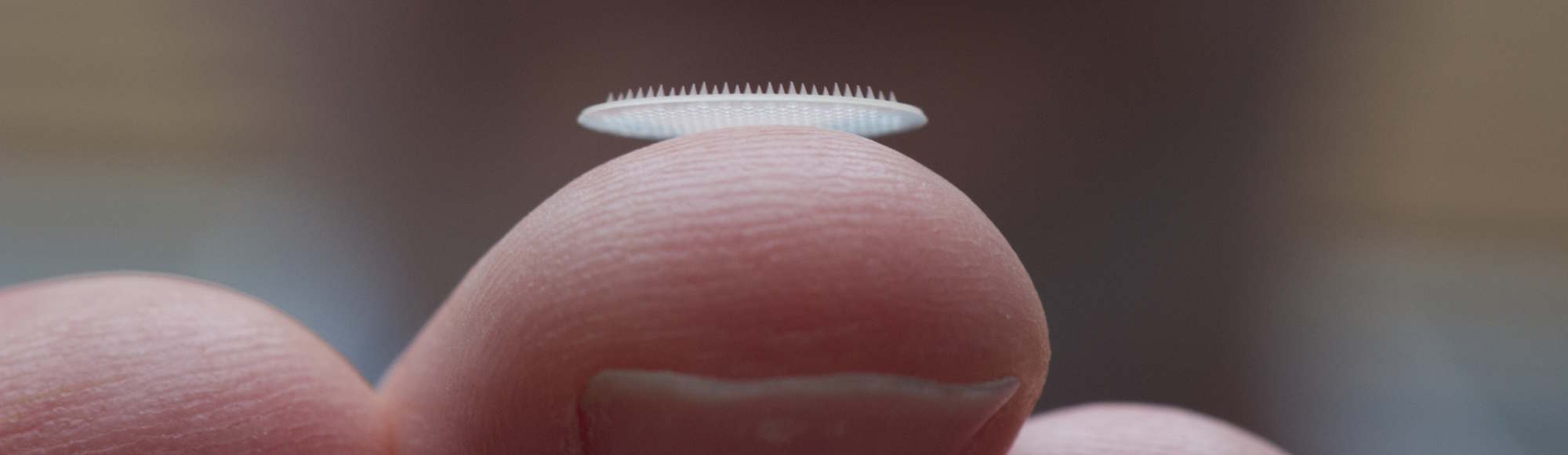
A Patch That Delivers Medicine for Months
Another of René Holm’s projects is progressing more smoothly – like the pretomanid work, it is being developed with support from the Gates Foundation, and it involves a small skin patch covered with microscopic needles. The needles penetrate only the outermost layer of skin and deliver a long‑acting drug from there.
Because the needles are just 400–600 micrometres long and never reach nerve endings, the patch is painless to apply. Beneath the skin, the microneedles dissolve and release tiny daily doses of medicine stored inside them.
Space is limited, so the technology is suited only to drugs required in extremely small quantities.
“There’s enough room for about six months of contraception,” Holm explains. “We think this could be a simpler, cheaper and more user‑friendly alternative to existing contraceptive methods.”
When Volume Becomes the Limiting Factor
Sometimes the obstacle isn’t particle size but sheer volume. There is a physical limit to how much liquid can be injected into the body before it becomes painful. Injections must go into muscle, and even the largest muscles – the gluteal muscles – can take no more than about 5 to 5.5 millilitres. In the shoulder, the limit is roughly 2 to 2.5 millilitres.
“Beyond that, it really starts to hurt,” Holm says. “And it shouldn’t.”
This is why medicines such as penicillin cannot be formulated as depot injections. There simply isn’t room for more than half a day’s dose in a single shot.
Whose Decision is it?
In the future, long‑acting medicines may be available for a wide range of chronic conditions, including dementia, epilepsy, depression, malaria and tuberculosis – potentially requiring injections only every six or twelve months.
That raises a final question: who should decide whether a patient takes daily pills or receives long‑acting injections?
For René Holm, the answer is straightforward: the patient.
“We’re not doing this for the system or the public purse,” he says. “We’re doing it for patients. And patients should choose the option that works best for them. Some people find reassurance in daily routines and frequent check‑ups. Others find relief in fewer injections. Depot medicines won’t replace tablets – they expand the choices.”
Meet the Researcher
René Holm holds two doctoral degrees and is Professor of Pharmacy at the Department of Physics, Chemistry and Pharmacy. He previously worked in the pharmaceutical industry at Janssen and Lundbeck and is co developer of 13 medicines that are now publicly available.